Language that Diminishes the Future
ANALYSIS
Language that Diminishes the Future:
The Repressive Psychiatric Discourse in 4.48 Psychosis
by Jinzhao Kan
“The depressive spell is a desperate cry for love.” -Sandor Rado1
Introduction
Sarah Kane ended her young life through suicide in 1999 at the age of 28, shortly after completing her last play 4.48 Psychosis. 4.48 Psychosis eschews a conventional plot; it presents itself as a mosaic of fragmented monologues, diagnostic lists, random numbers, etc.,2 that chart the mental landscape of a protagonist haunted by pathological grief.3 Besides, there is a striking reversal between what language conveys and what it accomplishes: the patient’s language, though expressing death and destitution, carries a plea for understanding, compassion, and the possibility of a liveable future;4 while the therapeutic language of the psychiatrist, though purporting to aid recovery, is signalling indifference, imposing unattainable socioeconomic demands, and foreclosing the possibility of that future.5
This piece examines these reversals in the clinical dialogue between the psychiatrist and the patient and argues, that care should begin not with correction towards a neoliberal norm but with attending to the patient’s present narrative of suffering.
Denial
This is the first of the seven patient-doctor dialogues in this play. In this dialogue, the psychiatrist continuously throws questions at the protagonist. This psychotherapeutic technique, known as Socratic questioning, is commonly applied in Cognitive Behavioural Therapy (CBT).6 The underlying premise of CBT is that “‘faulty’ thinking gives rise to anxiety and depression, rather than the other way around”, and the core philosophy of CBT is that “happiness depends not on what happens to us, but on how we interpret it”.7 Therefore, CBT’s approach involves using Socratic-guided discovery questions to identify and challenge various types of faulty thinking. However, this means that compliance with CBT could prevent patients from expressing certain thoughts and expressions that reflect their felt experience. In other words, the primary aim of CBT’s Socratic questioning is not an invitation to speak the language of feeling; it is a preparatory instrument for surfacing and disqualifying “faulty” cognitions, thereby licensing rectification at the level of the patient’s language, thought, and behaviour. In the scene that follows, the psychiatrist’s rapid-fire interrogatives operate exactly as this preparatory apparatus.

In this discourse, the protagonist’s lived reality is constantly denied by the psychiatrist’s ‘rational language’ – highlighting the blunt fact that the patient is not eighty years old. Although the protagonist tries to articulate her feelings with metaphor, the psychiatrist still insists on rectifying what he perceives as her false expressions by imposing a “rigid emotional-epistemological hierarchy which denies the depressive’s reality in favour of the reality of the positive or the ‘well’”.8 Moreover, instead of inviting the protagonist into such a ‘well’ way of thinking, this emotional epistemological hierarchy is enforced from the top down; violently and bluntly imposes his treatment agenda. According to the psychoanalyst Darian Leader, such “colonisation of value”, even if it is for the good of the patient, still “crush[es] a patient’s belief system by imposing a new system and policies on them”.9 Instead of leading the protagonist to find her own way of reconciling her experience, the clinical language forces the protagonist to leave her own interior life and immigrate into a healthy narrative, which our protagonist ultimately refuse to inhabit: “Your disbelief cures nothing. Look away from me”.10 Here, I am not suggesting that CBT’s approach is unacceptable or that the psychiatrist’s attempt to remove certain faulty thinking or values is unacceptable. Rather, I wish to highlight that these approaches should not justify overlooking or denying the patient’s authentic narrative and emotions. While some faulty thinking must be challenged and removed to help the patient overcome depression, it is still crucial to allow patients to recognise, understand, and gain greater control over their thoughts and emotions, rather than discarding them altogether.11
Responsibility
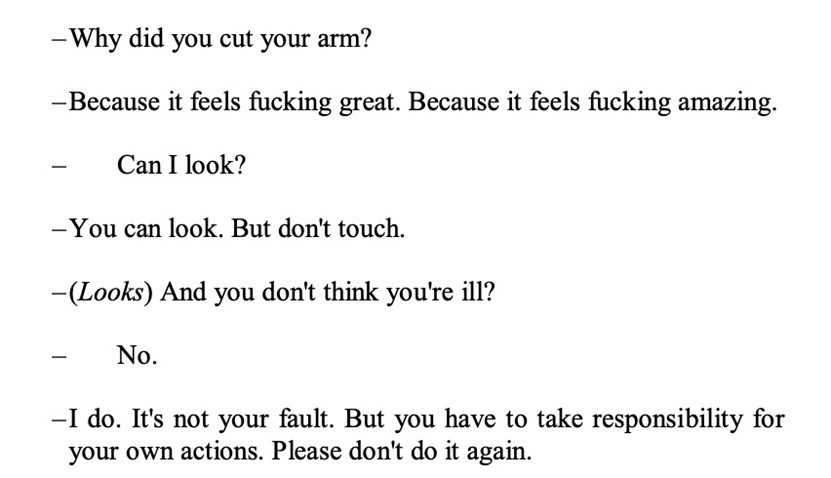
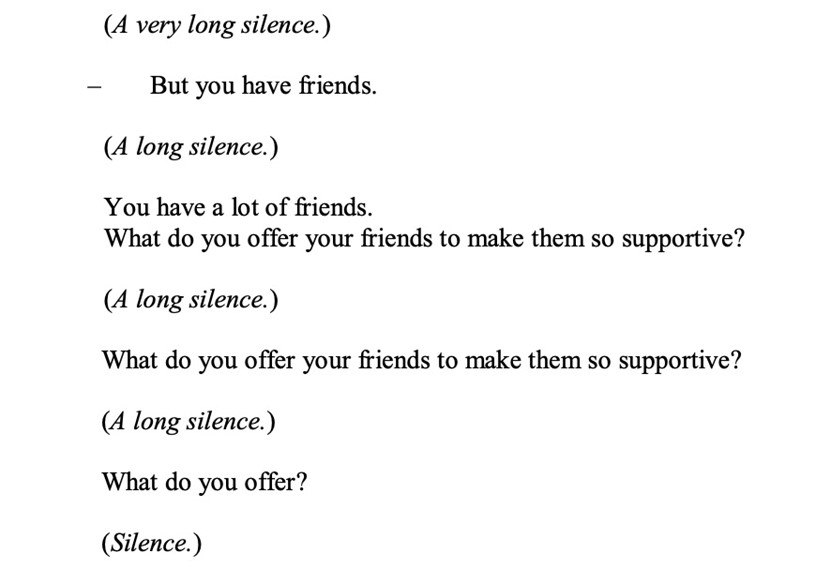
In this instance, besides denying the protagonist’s narrative and experience, the clinical language links her actions with concepts that carry moral weight, such as ‘fault’ and ‘taking responsibility’. There are benefits of saying “it is not your fault” and “take responsibility”, as they are viewed as being for the patient’s benefit – to prevent the protagonist from interpreting her suffering as the result of her own actions, which would be an unfair form of self-accusation, and to encourage her to take responsibility for suspending self-harming behaviour. However, the overwhelming repetition of these phrases also connotes the psychiatrist’s fundamental unwillingness to engage with the underlying motives behind the protagonist’s actions. While this may not reflect active hostility, it does suggest a clinical detachment that resists deeper understanding of the protagonist’s suffering. The protagonist protests that, “A room of expressionless faces staring blankly at my pain, so devoid of meaning there must be evil intent”.12 This dialogue focuses on the psychiatrist’s demand that the patient passively refrain from harming herself. The following dialogue explores how this demand shifts into an expectation that she actively submit to pharmaceutical intervention.
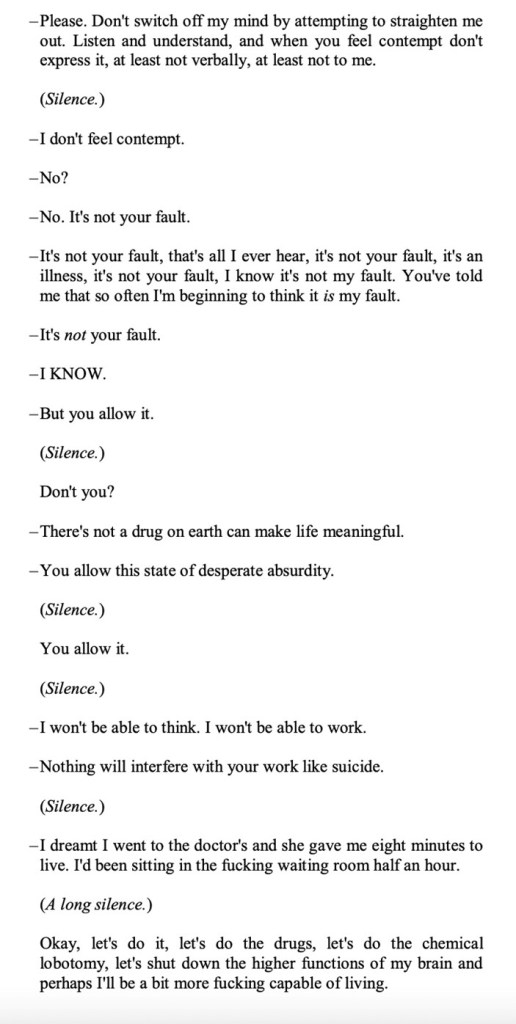
In this dialogue, the psychiatrist accuses her of having “allowed this state of desperate absurdity”. Apparently, the psychiatrist is suggesting that the protagonist remains in this dysfunctional state because she refuses to take antidepressants. By this interpretation, it is not the protagonist’s fault that she has ‘caught’ a mental illness; however, it would be her fault if she insists on receiving understanding from him while refusing his medical prescription. At the end of this dialogue, the protagonist surrenders to clinical power and begins taking antidepressants – an act that causes significant psychological and physical harm and, ultimately, leads to her suicide.
At this point, the foregoing explanations appear to clarify both the cause of this tragedy and the reversal of the language’s inherent purpose: an incompetent and indifferent psychiatrist, who, by adopting CBT—a method that inherently carries the flaw of ignoring and eliminating the protagonist’s narrative – prescribes antidepressants that inflict too much suffering for the protagonist to endure, leading her to end her life by overdosing on the very pills meant to cure her. However, such a superficial and reductive interpretation not only risks simplifying the complexity of her experience but also mirrors the psychiatrist’s own failure: to “understand” the protagonist merely in clinical or behavioural terms, rather than through the lived texture of her pain. As Kane indicated, “I’m dying for one who doesn’t care. I’m dying for one who doesn’t know”.13 To reduce the protagonist’s experience to a tragic clinical case would betray both the protagonist’s desperate attempts to articulate her reality and Kane’s expectation for us, as readers or audiences, to truly engage with the experience of mental suffering – not to explain it away, but to stay with it and to see beyond the words and symptoms. This tension is explored further in the next section.
Neoliberalism
What’s interesting about the concepts of ‘faulty thinking’ and ‘irresponsible behaviours’ that the psychiatrist adopts is that they are dialectical in nature – they cannot exist without their opposites: ‘not faulty’ or ‘correct’ thinking, and ‘responsible’ behaviours. However, the psychiatrist’s language in the play repeatedly denies the protagonist’s expressions while offering no clarification about what would count as the ‘right’ way of thinking and acting responsibly. Thus, the purpose of this section is to explain the normative values embedded in applied therapeutic languages, such as “it’s not your fault” and “take responsibility for your actions”.
In Leah Sidi’s account, 4.48 Psychosis exposes a neoliberal script in which clinical language redefines the patient as a self-managing economic actor; well-being is measured less by relief from pain than by restored productivity and the ability to resume work. To “recover” is to resume one’s position in the economic order, and depressive emotions are understood not as existential signals or cries for meaning, but as psychological “blocks” that obstruct one’s reintegration into the labour market. The imperative to “take responsibility”, in therapeutic discourse, is therefore not about moral autonomy or emotional ownership, but about taking economic responsibility through behavioural compliance and eventual employability.14 Under such a value system, the goal of treatment is to restore the patient’s economic productivity. Such a system marginalises any subjective expression of suffering that does not fit this model. The patient’s language is dismissed as “faulty thinking”, and her resistance is pathologised as “irresponsible behaviour”. In this light, the psychiatrist’s therapeutic language – such as “it’s not your fault” and “take responsibility” – becomes less a gesture of compassion and more an instrument of disciplinary normalisation, aimed not at understanding the patient’s psychic reality, but at restoring her economic viability within a neoliberal health economy.
On this reading, we can see why the psychiatrist persistently refuses the protagonist’s narrative: within a neoliberal clinic, many of her words and acts mark her as an insufficiently “self-responsible” subject – a subject who needs to be rectified. Self-harm and suicidal ideation are cast not as existential crises but as breaches of economic responsibility – “nothing will interfere with your work like suicide”15 – that must be eliminated. The psychiatrist’s language is strictly instrumental: her thoughts are “faulty” and must be corrected; her behaviours are “irresponsible” and must cease; refusal of medication is itself framed as further irresponsibility that mandates compliance. Nowhere does this discourse invite the articulation of feeling or the explication of pain. The result is a profound misalignment of ends: the psychiatrist’s speech acts aim to restore employable normality, while the protagonist’s language pleads to be understood. One vocabulary seeks the resumption of social function; the other longs, simply, to be heard.
Carl Jung asks in On Psychological Understanding, “how, out of this present psyche, can a bridge be built into its own future?”16 This question, quietly posed by Jung and dramatised viscerally in Kane’s play, urges us to reconsider what it means to heal – not only through compliance or correction in the name of restoring a liveable self-responsible future, but also by attending to the present moment with understanding, compassion, and a genuine commitment to alleviating psychic pain. Healing cannot be collapsed into a neoliberal teleology of reintegration – where care is audited by the speed of restored productivity – but must honour suffering as a present reality to be understood and witnessed. Such attention is impossible so long as compliance-driven clinical discourse drowns out the patient’s language. To build any bridge into the future, the therapeutic encounter must first dismantle the hierarchy that authorises one voice to speak over another. Such dismantling is not an end in itself but a precondition for any form of care that honours the patient’s lived experience rather than subsuming it under institutional aims. That is to say, healing cannot be reduced to a teleological process aimed solely at reintegration but must also honour the lived reality of suffering in its temporal immediacy – where pain is not simply a problem to be solved, but an experience to be witnessed.
JINZHAO KAN studied Philosophy at St Andrews (BA) and completed an MA in Philosophy, Politics & Economics of Health at UCL. His current interests are ethics and studies related to major depressive disorderS. Outside work, you’ll usually find him at the theatre or on a tennis court.
***
Edited by JOSH WEEKS
Proofreading by FLORA SAGERS
Lead image by Esteban Chinchilla via Unsplash.
Images of dialogues are taken from Sarah Kane, 4.48 Psychosis, in Complete Plays (London: Bloomsbury, 2001), 205, 211, 217-18, 220-21.
Categories